Omega 3 Fatty Acids
Copyright 2001 Krispin Sullivan, MS CN
Omega-6: Any of the fatty acids in the omega-6 family, short or long-chain. Also designated as n-6. These fats are polyunsaturates with multiple double bonds beginning on carbon 6.
Linoleic Acid: Short-chain omega-6 fatty acid also designated by LA. Can be converted into the long chain essential fatty acid arachidonic acid.
Arachidonic acid: Long-chain essential omega-6 designated AA
Omega-3: Any of the fatty acids in the omega-3 family, short or long-chain. Also designated by n-3. These fats are polyunsaturated with multiple double bonds beginning on carbon 3.
Linolenic Acid: Short-chain omega-3 fatty acid designated by ALA or LNA or alpha linolenic acid. May be converted into EPA but research suggests intake in humans will not increase the important DHA.
Eicosapentanoic Acid: Long-chain omega-3 designated EPA
Docosahexaenoic Acid: Long-chain omega-3 designated DHA. The most important fatty acid for human brain and heart function. Long thought to be conditionally essential, researchers now believe this is the MOST essential LCPUFA
Monounsaturated Fatty Acids: Fats containing one double bond on carbon 9. Designated omega-9 or n-9 or oleic acid.
Saturated fats: Fats with no double bonds. They can be short or long-chained. They are ubiquitous (in all life). Several are critically important to health and may be anti-viral and anti-bacterial. Natural saturated fats are stable to heat and light and safe for higher heat cooking. They do not oxidize readily.
Trans-fats: Trans-fatty acids are created when seed and grain oils are processed such as in the making of margarine and the hydrogenated fats used in most processed foods. Trans-fats also occur in vegetable and grain oils when they are heated.
Seed and grain oils: Corn, soy, safflower, sunflower, sesame, cottonseed, canola, walnut, peanut, flax,
Fruit oils: Olive, avocado.
Fatty acids play critical roles in human health and disease. Cell membranes (all cells) and mitochondria (found inside your cells at populations of 200-2000 per cell), are composed of a double layer of fats (bilipid layer). Your brain is about 60% fat. The fats you eat determine the health of your cell and mitochondrial membranes, including brain, heart, liver and kidney cells.
If cell and mitochondrial membranes contain damaged or inappropriate fatty acids cells so affected will be unable to perform their functions normally. Cell and mitochondrial membranes contain saturated fats, cholesterol, and a mix of n-9, n-6 and n-3 fatty acids. The mix is the magic. Too much of one or not enough of another fatty acid will lead to malfunction of the cell or cell death or cell uncontrolled multiplication (virus or cancer).
Research suggests our n-6:n-3 ratio in traditional cultures was 2-3:1 or even 1:1. Currently the dietary ratio in the US is calculated n-6:n-3 20-50: 1. As n-6 fatty acids are precursors to inflammatory processes in the human body and n-3 fatty acids precursors to anti-inflammatory processes it does explain the 75 million prescriptions for anti-inflammatory drugs each year and the $1.7 billion spent on over the counter anti-inflammatory medications. Globally NSAID sales topped $11.4 billion in 2014. We are in pain. We need good food and good fats.
Cholesterol is an alcohol, not a fat. Natural saturated fats are found in all foods to some degree. Saturation of a fat may be natural or from processing as is done to make margarine solid. Naturally occurring saturated fats are not associated with disease unless they are imbalanced by inadequate intake of the polyunsaturate essential fatty acids, especially the omega-3 fats.
Omega-3 fatty acids, DHA is essential to every cell in the human body, especially brain and heart cells. In cell membranes DHA enhances cell response (to insulin, neurotransmitters and other messengers) as well as sealing the cell membrane to prevent calcium overload WITHOUT using calcium channel blockers), and facilitate repair when cells are damaged. While omega-6 AA, arachidonic acid, is also essential for the brain and cellular immunity it is required in only small amounts. An excess of pro-inflammatory omega-6 fats contribute to cell membrane resistance, altering mood, insulin response, cognition and cell repair in a negative way.
Optimal daily intake of DHA (docosahexaenoic acid) in adult humans is 2,000 mg. Every day. Ideally supplement should contain MORE DHA than EPA. References available.
All mammals require DHA. Some anthropologists believe the human brain would not have developed as it did without access to high levels of DHA (docosahexaenoic acid) found in fish and shellfish and to a lesser degree in grass fed beef and wild game. Just two generations of high omega-6 and low omega-3 can lead to profound alterations in brain size and brain function in animals and probably in man. These scientists believe the human brain formed as it is today, large in proportion to body size because of abundance of DHA, and that its capacity is being diminished as the diet becomes deficient in omega-3 fats. Even if you regularly eat fish or take fish oil a relative omega-3 fatty acid deficiency can be created by an overabundance of omega-6 fats; a lack of omega-3 fats high in DHA; alcohol consumption; or the consumption of glycated or trans-fats. All of these conditions have been dramatically increasing in the US over the past 70 years.
Breast milk contains DHA and EPA only equivalent to amounts present in the mother's diet (what mom eats is critical). Many formulas contain added DHA however there is no standardization and formulas are never as nutritious as breast milk from a well fed mom. Raising children on formula or mother's milk deficient in omega-3 DHA contributes to impaired visual development, poor spatial development, slower learning, decreased comprehension and early allergies and asthma. OmegaQuant has an at home test, with a drop of breast milk, to check for sufficient omega-3 fats.
As of 2016 continued research is showing the critical importance, to our current health and our children's health, of reducing the amount of omega-6 fats in the American diet while increasing intake of omega-3 fatty acids, in particular docosahexaenoic acid, DHA. I have suggested the use of fish oil, butter, non-hydrogenated coconut oil and extra virgin olive oil for many years and this recommendation continues. To the basic fats I am now suggesting a minimum daily intake of fish or fish oils providing 2,000 mg or more of DHA along with whatever EPA is present.
Modification of fat intake should include identification and elimination of all 'added' omega-6 fats, trans fats, glycated fats and rancid/oxidized fats. Fish, shellfish, fish roe (caviar, fish eggs) and/or supplement omega-3 fatty acids need to be sought out and their intake substantially increased. To do this you will need to avoid processed foods, deli foods, foods subject to high heat cooking (fried, barbecued) as well as avoid grain and vegetable seed oils. Do not use sunflower, corn, soy, safflower, canola, or products that contain these oils. That is, no hydrogenated or partially hydrogenated fats, no margarine, no polyunsaturated vegetable oil of any kind, no shortening. and a low daily intake of nuts and seeds.
If you are not familiar with the term 'glycated' you may have heard of AGEs, Advanced Glycation End Products. When you get a Hemoglobin A1C test they are testing the amount of glycation in your blood. Glycation occurs in foods when they are subject to high heat (frying, browning, searing). In our bodies glycation occurs when sugars, glucose or fructose, interact non-enzymatically with fats and proteins creating Advanced Glycation End Products which damage cells and mitochondria throughout the body. The brown spots on the back of elderly hands are a visible glycation end product. These glycated fats/proteins lead to insulin resistance and neuropathies, are implicated in many types of cancer and contribute to all forms of dementia. Changing your source of dietary unsaturated fatty acids, low n-6, sufficient n-3 AND lowering your intake of all forms of sugar/fructose will protect your cells and mitochondria (and thereby you) from degenerative diseases, early aging and death.
Acceptable oils used in moderation and never subjected to high heat include extra virgin olive oil and avocado oil. Interestingly these are fruit oils. High oleic (omega-9) safflower or sunflower oils are also acceptable. Natural (non-hydrogenated) saturated fats are NOT a problem. Use butter, coconut oil, and non-hydrogenated lard, also in moderate amounts.
Fats in natural foods are never composed of a single type of fatty acid. Coconut oil has polyunsaturated fats and extra virgin olive oil and cod liver oil contain saturated fat. In nature fats are always mixed. Even fish oil contains saturated fat and cholesterol.
Naturally occurring cholesterol does not contribute to heart disease. Do not worry about total fat intake as long as it is from actual food, whole-fat milk, real butter, (preferably grass fed) the fat naturally found in wild caught fish, free range poultry and grass fed beef or pastured pork. The change to concentrate on is reducing ADDED FAT, eliminating as much omega-6 and processed fats as possible. Do your best to avoid all obvious omega-6 fats. If you suffer from obesity, diabetes, heart disease, autoimmune disorders, allergy, asthma, cancer, or any brain associated condition or injury, it is even more important that you increase your omega-3 DHA and EPA and avoid omega-6.
Between 1903 and 1998 added fats rose from 34 pounds per person per year, mostly butter and lard, to more than 66 pounds per person per year. All of the fat increase was in the form of omega-6 as salad dressing, margarine, shortening and hydrogenated fat added to processed foods and candies. See the charts that follow.
The ratio of omega-6 to omega-3 in the U.S. diet is somewhere between 25-50:1. The ideal ratio is somewhere between 3:1-1:1.
To correct this imbalance you will need to avoid added omega-6 fats and add fatty fish not less than 3 days a week making sure to eat the skin and fat under the skin. Remember, the fish should not be cooked with an omega-6 fat (vegetable oil or margarine) nor dipped in mayonnaise, also an omega-6 unless it is made with olive oil or Saffola Mayonnaise, high oleic containing mostly omega-9 fatty acids.
Regarding worldwide fish intake, from the WSJ, Dipietro, April 2014
The average U.S. consumer ate 14.4 pounds of seafood in 2012, the last year for which figures are available, down from 15 pounds in 2011 and a record high 16.6 pounds consumed in 2004. That's far less than the average 82 pounds of chicken, 57 pounds of beef and 46 pounds of pork. Americans consume in a year. It's also much less than the amount of seafood eaten in other countries. The average Japanese consumer eats 120 pounds a year, while Spaniards consume 96 pounds.
If you are not eating fatty fish such as mackerel, sardines, salmon, daily, including the skin and fat under the skin, you will need to use a fish oil supplement containing a minimum of 2,000 mg DHA plus whatever amount of EPA it contains (equivalent to about 1-2 tbsps. of fish oil). I mention skin and fat under the skin as this is a primary storage site for fish fat. Often the flesh/muscle is quite lean, low in omega-3 content.
Fish may can be taken with or without food. Many clients find that there is less reflux when taken on an empty stomach. If you have a sensitive stomach do not take all of your fish oil at once. "Enteric Coated" may be especially problematic. I am not sure why manufacturers do this but sensitive stomachs don't handle enteric coated well and it may result in diarrhea. If taking your oil all at once seems to much split your daily amount into two doses. Do not take any after 5 PM if you find the fish oil very energizing as it may disrupt your sleep. If digestive upset occurs stop until things normalize and increase slowly or stick with a lower dose. If you use the soft gels, keeping them in the freezer will keep your oil fresher AND it seems to prevent burping and gastric distress.
The maintenance dose of fish oil for most adults is a minimum of 2,000 mg of DHA. All fish oil supplements contain both DHA and EPA, so as long as the oil is near balanced, nearly equal DHA and EPA, you will get sufficient EPA. Depending on diet, genetics and body size, one might need a little as 1500 mg DHA (plus naturally occurring EPA). The current guidelines for infants, children and adults is to prevent overt deficiency NOT the optimal sufficiency dose.
Getting a tablespoon of Carlson Cod Liver Oil daily would provided 1500 mg DHA and 1200 EPA and provide safe and adequate amounts of A and D for most adults and children. A teaspoon is likely appropriate for infants. To get the required 2,000 mg for adults consider the Cod Liver Oil plus two Now Foods DHA-500. Other choices are available. Just make sure the amount of DHA is greater than EPA and that you take enough of the supplement to get the full 2,000 mg. DHA or a bit more.
Some supplements contain a lot of EPA and not much DHA. I would not suggest these supplements, avoid. DHA is essential. EPA is not essential. NEVER BUY A FISH OIL SUPPLEMENT CONTAINING MORE EPA THAN DHA.
The best source of omega-3 fish oil is one you will take daily.
Membrane phospholipids require fatty acids, including AA, EPA and DHA. The membrane phospholipid in both heart and brain will preferentially contain DHA, but only if enough is present in the diet. Pretty important.
Phospholipids, present in all cell and mitochondrial membranes, are also essential and are found naturally in milk fat, organ meats including brain, heart, liver and kidney, egg yolks and fish eggs. The important phospholipids include phosphatidylcholine, phosphatidylinositol, phosphatidylethanolamine and phosphatidylserine. You may benefit from additional supplementation. If eggs are used they must be from free ranch chickens raised with natural foods and love. All fish products must be wild caught NOT farmed. Farmed fish are fed omega-6 fats making them miserable and sick and thereby also you.
If you don't eat any or eat little of the above consider lecithin granules. They contain all of the essential phospholipids in significant amounts. 1 heaped tablespoon of lecithin granules (which while derived from soy contain NO soy lectins, or use the sunflower lecithin) provide all of the phospholipids required by humans.
The granules are best kept in a dark dry cupboard, taken by the tablespoon directly in the mouth just before or after your daily fish oil or fish meal. They don't mix well with any liquid. Do not chew them as they will bind firmly to your teeth. I prefer soy lecithin because it has a better 'human' profile of phospholipids than sunflower seed lecithin. My favorite brand is Fearn because each can has been consistent in production. Some other brands, on occasion, seem to have been exposed to excess moisture causing off flavor and color. The phospholipids are still intact but less pleasant to take daily.
Make sure to read the magnesium page. Magnesium must be sufficient for combining omega-3 with phospholipids. Things 'go together' and won't work unless all parts are present.
For your daily DHA with EPA I routinely suggest Carlson Cod Liver Oil 1 tablespoon PLUS 2-4 of the Now Foods DHA-500. Almost all fish oil concentrates are ethyl esters which clinically do work but aren't 'fish oil' with naturally occurring glycerolipids. The cod liver oil has the natural fish fats, as well as A and D and DHA and EPA for a great combination. Carlson has reduced the amount of vitamin A, just 2550 in a tablespoon, so for most it is safe, as long as you are not taking high doses of vitamin A and/or D in another supplement or, as one client from years ago did, eating goose liver pate daily, massive amounts of A.
Omega-3 and omega-6 fats move rapidly into cell membranes, including the membranes of nerve and epithelial cells. Epithelial cells compose skin, the lining of the arteries and lungs, the linings of the ducts in the breast and testes. The preferential fat for these brain and epithelial membranes is omega-3 DHA but n-3 will be replaced by n-6 DPA if sufficient n-3 is not available. Cells where omega-3 is displaced by omega-6 suffer from inflammation and are less able to repair themselves and over time may become hyperplasic (pre-cancerous).
The brain and nerves so need omega-3 that they will rob it from every other cell to maintain optimum brain levels. Some of the brain and nerve conditions associated with high omega-6 and/or low omega-3 include, alcoholism, depression, manic depression, memory loss, impaired night vision, anxiety, insomnia, Multiple Sclerosis, Alzheimer's, Parkinson's, ADD/ADHD, dyslexia, stress induced hostility and schizophrenia.
In the following graph of US per capita fat consumption 1909-1998 it is clear that both our overall intake of fats and intake of omega-6 fats has dramatically increased. From this data it seems prudent to reduce omega-6 fats and increase n-3 DHA.
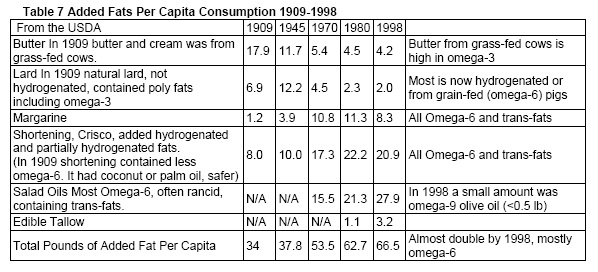
There is no indication our intake of natural saturated fats has increased over this period of time as is suggested to be the commonly accepted 'cause' of degenerative diseases. What has increased is our intake of processed omega-6 fats and an imbalance between n-6 and n-3..
The following paper was presented in 2000 at the National Institute of Health is Washington, DC. The BOLD text is my emphasis. Keywords in understanding fats- Linoleate is omega-6, linolenate is omega-3 as is DHA and EPA and oleic is omega-9. Linoleate, DHA, EPA and linolenate are all polyunsaturated fats. Oleic omega-9 is monounsaturated fat.
Mizuhoku, Nagoya 467-8603, Japan
Excessive linoleic acid (omega-6) intake and relative n-3 deficiency syndrome
Animal experiments and epidemiological studies have revealed that excessive intake of linoleic acid (omega-6) (LA, n-6) is a major risk factor for cancers of western type, allergic hyper-reactivity, coronary heart disease ( CHD) and cerebrovascular disease (CVD) (1). Although epidemiological studies performed in the USA failed to reveal a positive correlation between LA intake and breast cancer mortality, this is probably because the proximate marker for breast cancer is the proportion of n-6 eicosanoid precursors in phospholipids, which is saturated both in the high and low LA intake groups in the USA. Empirical equations presented by Lands indicate that both increasing the intake of n-3 fatty acids and decreasing that of n-6 fatty acids are necessary for effectively decreasing the n-6 eicosanoid precursors in phospholipids and thereby decreasing cancer mortality. On the other hand, high n-6/n-3 ratio but not hypercholesterolemia has been proved clinically to be a major risk factor for thrombotic diseases. Over-production of inflammatory lipid mediators of n-6 series has been shown to be a major cause for the rapid increase in allergic hyper-reactive patients in Japan.
President's Summary 1997 from the Japan Society for Lipid Nutrition
After discussion through several annual meetings of the Japan Society for Lipid Nutrition, Presidents Summary 1997 was published (in Japanese) as a review article (J. Lipid Nutr. 6:5-42, 1997), in which 20% as total fat energy was recommended for those with moderate physical activity. For healthy populations, saturated plus monounsaturated : n-6 : n-3 = 2.5 : 0.8 : 0.2 (n-6/n-3 4) was recommended.
For the primary and secondary prevention of those diseases described above, an n-6/n-3 ratio of 2 was recommended. The latter value was based on: 1) even the n-6/n-3 ratio of Danes was 3 in a well known epidemiology of Greenland natives; 2) the ratio of current Japanese is 4 but the incidence of cancers of western type has been increasing rapidly, and the ratio of 4 or above cannot be recommended; 3) animal experiments have shown the effectiveness of decreasing n-6/n-3 ratio to below 2 for the suppression of carcinogenesis and metastasis; and 4) the safety of n-6/n-3 ratio of 1 has been established in animal experiments and in a retrospective study on hunters and gatherers foods.
In order to meet the recommendations described above, vegetable oils with n-6/n-3 ratios of 2 or below and those with very low n-6 fatty acid contents (e.g., high-oleic type) are useful. However, there was another criterion to be considered; the presence of minor components, which affect animal physiology seriously.
Survival time-shortening and renal injury induced by some vegetable oils and partially hydrogenated oils in SHRSP rats
Using soybean oil as a control, some oils were found to prolong the mean survival time of SHRSP rats by ca 10% (e.g., DHA-rich fish oil, perilla seed oil, flaxseed oil) while some others shortened it dose-dependently by ca 40% (double-low rapeseed oil, evening primrose oil, high-oleate safflower oil, high-oleate sunflower oil, olive oil and partially hydrogenated rapeseed and soybean oil). When the rapeseed oil was lipase-treated, the resulting free fatty acid fraction was almost free of such activity, indicating that the survival-time shortening activity is due to minor components other than fatty acids in these oils. Free fatty acid fraction from partially-hydrogenated soybean oil exhibited a survival time between those of the original oil and soybean oil. It should be emphasized that lard and sesame oil were relatively safe for the SHRSP rats.
Those oils with survival-time shortening activity were found to cause renal injury; lesions in blood vessels, accelerated proteinuria, decreased platelet count and elevated gene expression for TGF7, fibronectin and renin.
Choice of n-3, monounsaturated and trans-fatty acid-enriched oils
In order to decrease the n-6/n-3 ratio of our current foods to 2 or below, the intake of high-n3 linolenate oils such as perilla seed oil and flaxseed oil as well as seafood and vegetables should be increased.
My note here- At the time of this study it was believed humans could readily use and convert ALA (perilla, flax) to longer chain fatty acids. For most in the US this is not true. We need seafood. We require fish fat.
High-linoleate (omega-6) oils are inappropriate for human use as foods. For deep-frying and preservation purpose, high-oleate vegetable oils are useful but all the high-oleate vegetable oils and hydrogenated vegetable oils we have examined so far exhibited the survival time-shortening activity, and I cannot recommend people to have these oils in large quantities. Instead, lard was safe for this animal model, and could be used in quantities not to induce obesity; animal fats as well as a high-LA vegetable oil intake caused insulin resistance in a NIDDM model of rats.
Reference
Okuyama, H., Kobayashi, T., and Watanabe, S. (1997) Dietary fatty acids: The n-6/n-3 balance and chronic, elderly diseases. Excess linoleic acid (omega-6) and relative n-3 deficiency syndrome seen in Japan. Prog. Lipid Res. 35: 409-457.
HDL has long been known as the good cholesterol, protecting against heart disease and atherosclerosis. It was recently discovered that HDL has powerful antioxidant properties similar to vitamin C, vitamin E, and coenzyme Q-10. An HDL associated enzyme, lecithin-cholesterol acyltransferase , which forms part of HDL, is a powerful antioxidant enzyme that blocks the oxidization of LDL cholesterol. Cholesterol is beneficial and without harm if it is not first oxidized. Vohl MC, Neville TA, Kumarathasan R, Braschi S, Sparks DL: A novel lecithin-cholesterol acyltransferase antioxidant activity prevents the formation of oxidized lipids during lipoprotein oxidation. Biochemistry; 1999 May 11;38(19):5976-81
Oleic acid is an omega-9 such as found in olive oil and avocado oil. Some sunflower and safflower oils are bred to be high in this fat, safe for cooking and mayonnaise. Look for the words High Oleic on the bottle and a high number for omega-9 on the label.
Fatty acids are the "building blocks" of all cell and mitochondrial membranes. You have about 37.2 trillion cells in your body at any given time (cell death/cell renewal). Mitochondria are currently uncountable BUT one healthy liver cell contains about 2,000 mitochondria, muscle cells several hundred per cell depending on how much you exercise, more exercise stimulates more mitochondria. Big numbers. All require fats as cell and mitochondrial membranes are encased in a bilipid layer (two layers of phospholipids, lipids being the fat part). Some fatty acids required to build these cell and mitochondrial membranes, which include neurotransmitters, hormones and immune cells are called "essential" because your body needs them, yet cannot make them; you must eat them. As cells and mitochondria are always in the process of birth and death (even when you are old) you need these essential fats every day.
Omega-3 fatty acids and omega-6 fatty acids come in short and long chain configurations.
The short-chain omega-3 is alpha-linolenic acid (LNA or ALA). Its elongated derivatives include: eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and a few others, less well known and less studied.
The main short-chain omega-6 is linoleic acid (LA). Like LNA, it also has elongated derivatives, the main being arachidonic acid, necessary for prostaglandin formation and brain function. Linoleic acid from whole foods, nuts, seeds is essential, but in amounts that are moderate. Linoleic acid containing foods should never be heated above 250 degrees. Heat oxidizes and glycates linoleic acid. Linoleic acid and AA may also be glycated which results in cell membrane damage from oxidation. High amounts of glycated fatty acids result in oxidation of LDL fractions is blood (associated with heart disease).
The very long-chain omega-3 EFAs (especially DHA) are connected with brain and visual development in infants AND adults. Deficiencies in adults can lead to impaired mental processes, including learning disorders, dementias and other neuronal diseases, impaired vision, and depression. Studies suggest that prolonged deficiencies might lead to retinal and macular damage. In pregnant women low levels of the elongated omega-3 can actually reduce brain size in offspring and brain shrinkage in the new mom.
How much of these essential fatty acids do you need? Many sources suggest Americans do not get enough omega-3. Even worse we get too much omega-6, which displaces omega-3 in cell membranes, mitochondria, and neural circuits.
Researchers involved in the Workshop on the Essentiality of and Recommended Dietary Intakes for Omega-6 and Omega-3 Fatty Acids suggest "adequate intakes" of each:
The problem with these numbers is that a diet containing nuts and seeds or meat or even milk and eggs as a protein source has at least 12 grams of omega-6. That would mean that a minimum (not optimal) of omega-3 would be 1.95 grams which is the amount in about 6 ounces of fatty fish daily (more would be needed if lean fish is used) however, even that won't work if you are eating farmed fish. Farmed fish is poor in omega-3 and high in omega-6. Farmed fish also contains higher levels of toxins than wild caught fish.
Research since the Workshop suggest the ideal daily intake of DHA is more likely 1500-2,000 mg daily. EPA is NOT essential and cannot be converted into DHA. DHA in excess is easily converted into EPA.
Sources looking at the dietary ratio of omega-6 to omega-3 fatty acids suggest that in early human history the ratio was about 1:1. Currently most Americans eat a dietary ratio that falls between 20:1 and 50:1. The optimal ratio is most likely between 3:1 and 1:1. For most Americans this means greatly reducing the omega-6 fatty acids they consume and increasing the amount of omega-3 fatty acids.
As mentioned there are other fat issues, glycated fats, rancid fats, trans-fats or hydrogenated fats. Do your best to avoid them. These damaged fats are not good for you but neither are the 'cold pressed' so called healthy vegetable oils high in n-6, like canola, soy, safflower, sunflower or corn oils. If you are vegan or vegetarian you could use flax or perilla oil however these highly unsaturated fatty acids are damaged by heat, light and oxygen so beware of rancidity. You can get all you need of n-6 and n-9 fatty acids from food. See note on vegan/vegetarian issues below.
The best source of omega-3 fatty acids is cold-water (the colder the better) fish and fish eggs (yes, caviar) high in both EPA and DHA. You may need as little as three servings a week of very fatty fish (make sure to eat the skin and surrounding fat) or 8 or more ounces daily to meet your genetic need. If fish are not your thing you may use fish oil liquid or soft gels. The suggested daily dose is 2,000 mg DHA for most adults along with some EPA. Some load, taking 2500 -3000 mg DHA for 1-3 months under certain circumstances, recovery from injury, illness, surgery or if diabetic or obese. Maintenance for most persons, unless you consume fatty fish regularly, would be combined EPA and DHA with DHA being 2,000 mg daily. This dose will only produce positive results if glycated fats and a high intake of omega-6 fats are avoided ongoing.
Supplemental EPA fish oils may increase the production of free radicals in your body. DHA turns out to be an antioxidant so getting higher amounts of DHA will protect from EPA oxidation. Do always get sufficient antioxidants, particularly vitamins D, K, A and E along important when you increase fish oil intake. All four vitamins are fat soluble. Do take with a meal containing fat OR with your dose of fish oil. If you get your omega- 3 from fish and fish eggs or cod liver oil the necessary antioxidants will be in your food.
Vegans/Vegetarians- You may believe your foods or supplements will contain sufficient LA (linoleic acid- omega-6 elongated to AA) and ALA (alpha-linolenic acid- omega-3 elongated to EPA) rather than consuming meat/poultry/eggs/fish containing AA, EPA and DHA. You should be aware long chain PUFAs are not found in vegetables, grains, nuts, seeds and other non-dairy, non-meat/poultry/fish sources. The ability of humans to convert short chain PUFA into the longer essential AA, EPA and DHA is determined by your genes. Even if you are one of the few able to convert, conversion is further reduced in aging. Lack of essential AA and DHA will hasten inflammation, degeneration and death. A study published in MBE March 2016 found-
...LCPUFA can be obtained directly from animal foods or synthesized endogenously from 18 carbon precursors via the FADS2 coded enzyme. Vegans rely almost exclusively on endogenous synthesis to generate LCPUFA and we hypothesized that an adaptive genetic polymorphism would confer advantage. The rs66698963 polymorphism, a 22 bp insertion-deletion within FADS2, is associated with basal FADS1 expression, and coordinated induction of FADS1 and FADS2 in vitro. Here we determined rs66698963 genotype frequencies from 234 individuals of a primarily vegetarian Indian population and 311 individuals from the U.S. A much higher I/I genotype frequency was found in Indians (68%) than in the U.S. (18%)...
The gene study just looked at the essential AA (arachidonic acid) not the also essential DHA (docosahexaenoic acid).
EPA, DHA and AA are converted from shorter chain essential fatty acids. The ability to do so is GENE based. If you don't have the genes or they are not fully functional you will suffer from LCPUFA deficiency which will result in multiple health issues and decreased longevity. Your ancestors determine the success of your current dietary choices. Choose wisely.
In many studies even large doses of ALA (flax or perilla) did not raise membrane DHA. OmegaQuant testing has found no increase in DHA in persons using any source of ALA. Flaxseed, perilla oil and walnuts are common sources of ALA. Moderate amounts of ALA may be beneficial however recent studies suggest high amounts of ALA may be associated with prostate cancer. Other studies suggest ALA is easily damaged (oxidized) leading to cell membrane deficits.
Low levels of DHA are strongly associated with many types of cancer as well as heart disease, obesity, diabetes, depression, IBS, IBD, colitis, allergies and autoimmune diseases.
For most humans fish fat is an essential food. If you do not want to use fish or fish oil consider the OmegaQuant testing to determine if you are able to remain healthy consuming your current dietary choices.
A sampling of foods high in DHA and EPA (combined):
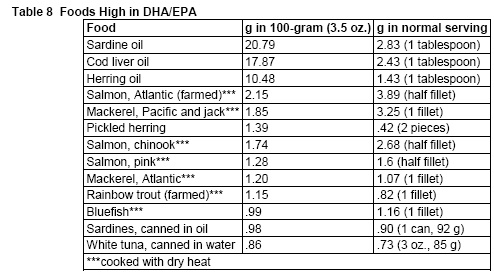
Sardines are high in EPA as are anchovies. Sardine oil is not a good source of DHA. Sardine oil is a less expensive source of fish oil. Supplements containing it are often imbalanced with too much EPA. Your heart and brain and other organs, liver, kidney, REQUIRE DHA.
Omega-6 AA (arachidonic acid) is an essential fat. We require it. However we need only a bit every day easily found in whole milk products (avoid non-fat dairy please), lean meats, eggs and poultry. Better sources include grass fed beef, range fed chickens and wild game. Do include organ meats as they contain essential phospholipids as well as essential fatty acids. .
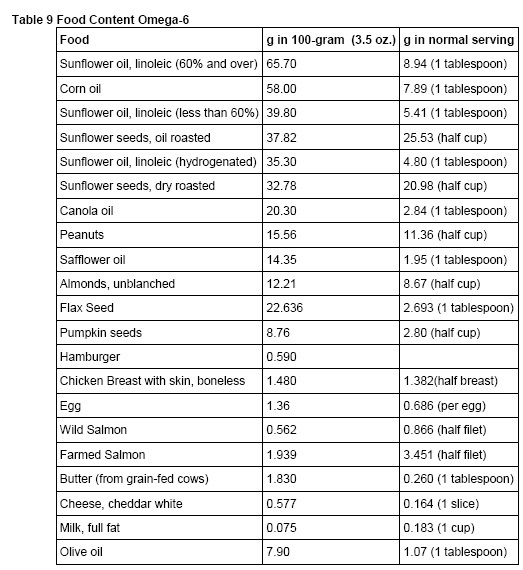
Many Americans get our omega-6 fatty acids from vegetable oils including prepared/processed foods made with vegetable oils, and margarine, Crisco and mayonnaise. The popular evening primrose and borage supplements are also high in omega-6. As you can see from the chart below, simply changing the type of oil you use could greatly reduce your intake of LA. Also pay special attention to the difference between wild and farmed salmon as to omega-6 content. This pattern of higher omega-6 in farmed/domesticated animals is repeated in wild compared to domestic game, grain-fed compared to grass-fed beef, and standard compared to pastured poultry and pork. Organic dairy, meat and poultry are often from animals fed grain so the n-6:n-3 will still imbalanced. Organic does not mean grass fed or free range.
.
Vitamins E and K, Protecting Cell and Mitochondrial Membranes
A typical breakfast in Tokyo, Japan contains natto, fish, rice and fermented pickles. Natto is high in vitamin K. The fish, consumed flesh, bones and skin, contains vitamin K, vitamin D, omega-3, minerals and amino acids. The pickle improves digestion. In all traditional cultures the daily diet contains protein, including fish, fish eggs, and organ meats, all excellent sources of essential phospholipids, dark greens and some fermented food from natto to yogurt to fermented cabbage. This wide variety assures adequate nutrition from fresh whole foods. Without this natural balance nutritional deficiencies are inevitable.
Vitamin K is a fat-soluble vitamin found in dark green leafy foods and naturally fermented foods. The symbol K is used for potassium on the periodic chart. We are not talking about potassium here, but a fat soluble vitamin. Vitamin K1 is phylloquinone, found in plants. Vitamin K2, menaquinone, is found in animals and made in the human gut by 'good' bacteria. Antibiotics may limit our ability to make K in the gut. Probiotics like acidophilus may restore gut K production. There is increasing evidence that natural gut production is not enough to support artery and bone health. Dietary sources are critical.
Vitamin K reverses postmenopausal bone loss by keeping calcium in the bone where it belongs, working better than Fosamax. Low levels of vitamin K lead to under-carboxylated calcium forming plaque in the arteries in heart disease. K is necessary for the formation of osteocalcin a bone builder. It is intimately related to the functions and actions of vitamin D. Vitamin K is an effective anti-oxidant in the cell membrane and necessary for normal blood clotting.
Large doses of the naturally occurring K1 and K2, up to 45 mg daily, have been given with few side effects, to treat various cancers. Normal, traditional dietary doses (1-5 mg) of vitamin K as found in naturally fermented foods, dark green leafy vegetables, seaweeds and animal livers, do not 'over' coagulate the blood. Adequate vitamin K normalizes fragile membranes. It has proven useful preventing or correcting easy bruising, varicose veins and 'spider' veins. Vitamin K within physiological amounts does not make blood thicker or 'stickier'.
K toxicity has occurred in infants given vitamin K3 (not a natural form of K) by injection. In research, only the analog 'man-made' K3 has shown toxicity.
If you are on a blood thinning medication, such as Coumadin or aspirin or other non-steroidal anti-inflammatory, you must discuss vitamin K supplementation with your physician. Some of these medications work by destroying vitamin K factors, not a good thing in the long term. Recent research suggests Coumadin may, by way of reducing vitamin K, induce arterial calcification. Some researchers are now suggesting a vitamin K supplement for Coumadin users.
Med Res Rev. 2001 Jul;21(4):274-301.
Arterial calcification: a review of mechanisms, animal models, and the prospects for therapy.
Wallin R, Wajih N, Greenwood GT, Sane DC.
Section of Rheumatology, Department of Internal Medicine, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA.
The causes of arterial calcification are beginning to be elucidated. Macrophages, mast cells, and smooth muscle cells are the primary cells implicated in this process. The roles of a variety of bone-related proteins including bone morphogenetic protein-2 (BMP-2), matrix Gla protein (MGP), osteoprotegerin (OPG), osteopontin, and osteonectin in regulating arterial calcification are reviewed. Animals lacking MGP, OPG, smad6, carbonic anhydrase isoenzyme II, fibrillin-1, and klotho gene product develop varying extents of arterial calcification. Hyperlipidemia, vitamin D, nicotine, and warfarin, alone or in various combinations, produce arterial calcification in animal models. MGP has recently been discovered to be an inhibitor of bone morphogenetic protein-2, the principal osteogenic growth factor. Many of the forces that induce arterial calcification may act by disrupting the essential post-translational modification of MGP, allowing BMP-2 to induce mineralization. MGP requires gamma-carboxylation before it is functional, and this process uses vitamin K as an essential cofactor. Vitamin K deficiency, drugs that act as vitamin K antagonists, and oxidant stress are forces that could prevent the formation of GLA residues on MGP. The potential role of arterial apoptosis in calcification is discussed. Potential therapeutic options to limit the rate of arterial calcification are summarized. Copyright 2001 John Wiley & Sons, Inc.
Curr Opin Nephrol Hypertens. 2002 Jul;11(4):437-43.
Erratum in: Curr Opin Nephrol Hypertens. 2003 Mar;12(2):221.
Novel mechanisms in accelerated vascular calcification in renal disease patients.
Demer LL, Tintut Y, Parhami F.
Departments of Medicine and Physiology, UCLA School of Medicine, Los Angeles, California, USA. ldemer@mednet.ucla.edu
PURPOSE OF REVIEW: Vascular calcification occurs more often and earlier in patients with end-stage renal disease than in normal controls. It is a regulated biological process following many of the cellular and molecular programs in osteogenesis. This review summarizes some of the regulatory mechanisms that may explain its severity in renal patients. RECENT FINDINGS: A subpopulation of cells from arteries and cardiac valves produce a mineralizing matrix and undergo osteoblastic differentiation. Osteogenic differentiation regulators are found in calcified but not normal arteries. Phosphate levels have dramatic effects on vascular calcification in vitro, through a sodium phosphate transporter signaling molecular changes. Atherogenic oxidized lipids promote osteoblastic differentiation of vascular cells and inhibit bone mineralization. In uremic patients, the severity of dyslipidemia corresponds with the progression of vascular calcification. Oxidative stress and inflammatory mediators may underlie the effects of oxidized lipids. In dialysis patients, the degree of cardiac valvular calcification corresponds with levels of C-reactive protein. Genetic factors may also contribute. Polymorphisms of the inflammatory adhesion molecule, E-selectin, associate with coronary calcification in young women. Mice deficient in matrix GLA protein, which inhibits bone morphogenetic protein activity, develop complete ossification of the aorta, presumably as a result of unopposed osteogenic activity on vascular mesenchyme. Since matrix GLA protein function requires gamma-carboxylation of its glutamate residues by a vitamin K dependent carboxylase, warfarin treatment may affect vascular calcification by blocking vitamin K and hence matrix GLA protein activity. SUMMARY: These findings indicate that vascular calcification is regulated both positively and negatively by a wide variety of mechanisms affecting patients with renal disease.
Research demonstrates a high intake of fat, whether omega-3, omega-6, omega-9, or saturated fat, increases the need for vitamins Gamma E-Complex and K. If you include glycated fats in your daily diet consider an additional carnosine supplement daily. The traditional diet would provide extra nutrients as a natural component of the fatty food.
Food processing and storage change the availability of these natural components. In animals given diets high in omega-3, omega-6, omega-9 or saturated fat, liver content of vitamin K was reduced to 1/5 of controls (normal chow diet).
In the US vitamin E supplementation is common. Most health food store multiples contain 100-200 IU d-alpha tocopherol per daily dose. I prefer Gamma E Complex at not more than 200 IU daily. Higher levels of E have a reverse effect. In fact, high levels of E actually reduce levels of vitamin K, not a good idea for postmenopausal women needing to keep or rebuild bone or heart patients using omega-3 and vitamin K to prevent or reverse arteriosclerosis.
Finding vitamin K is much harder, whether in foods or in a supplement. The DRI is 90 mcg. but just 1 mg (1,000 mcg, more than 10 times the DRI) has reversed bone loss in post-menopausal women, reducing urinary calcium loss by 25% within a few days of starting supplementation. 10 mg (10,000 mcg) of vitamin K MK-4 daily has been used by our space program to prevent bone loss in astronauts during weightlessness. MK-4 45 mg has been used successfully to treat some types of cancer in Japan.
A study published April 2001 in Kardiologie correlated low levels of vitamin K to under-carboxylated MGP (a protein that reflect artery health). The conclusion? Low levels of K allow calcium to leave the bone, not be delivered to the bone and promote the deposition of calcium in soft tissues. The study determined the lowest level of vitamin K to reach sufficiency is 900 mcg, just under 1 mg.
Vitamin K works with vitamin D (both are equally important) to prevent bone loss and build new bone. It also influences blood sugar levels and adult onset diabetes. Low vitamin K contributes to post meal hyperinsulinemia (high insulin) and insulin resistance.
We do make some vitamin K in our guts if we have normal bowel flora (the 'good' gut bugs, they make the K for us) and normal bowel function. Constipation, diarrhea, IBS or Crohn's would all indicate a problem with vitamin K, either making it or absorbing it. Dietary fiber (soluble fiber) helps the 'good' gut bacteria thrive so soluble fibers, found in high fiber foods like berries, figs and some legumes, will increase vitamin K if the gut bugs are right.
Vitamin K1 is found in very dark green leafy vegetables like chard, spinach, bok choy and seaweeds such as dulse. Vitamin K2 is found in beef and poultry livers.
Vitamin K MK-7 NutriZing is 600 mcg. Dose is one a day with a fatty meal. High dose MK-4 is also available from Life Extension Mega K2 (45 mg of MK-4). Very high dose so best to use under supervision of your healthcare practitioner.
To be absorbed vitamin K, in a supplement or in food, must be consumed with fat. Fat-free veggies for dinner, no K (or beta-carotene) absorbed, but with a little added butter or extra virgin olive oil on your greens the K is very well absorbed. Sushi, wrapping fish in seaweed, gives a meal high in vitamin K and omega-3, both well absorbed. This rule regarding the need for fats to absorb is also true of 'green drinks'. Unless you add fat to your drink or have some with it (not later) the important fat-soluble nutrients will pass you right by.
Vitamins A, D and E also need fat for absorption. Since they are usually found in a fat containing supplement (cod liver oil) or in fats found in animal or poultry livers, butter, full-fat dairy and such, absorption is not a problem. Our modified 'low-fat' or 'no fat' diets are un-natural and rob us of the very important fat-soluble vitamins, A, D, E and K. Absorption of calcium, A and D from non-fat milk or other non-fat dairy products is poor.
If you have difficulty digesting fats it is important to address this problem ASAP. Health and longevity require adequate A, D, E and K and all essential phospholipids. Without good fat digestion you will not get what you need, from supplements or from food.
Essential and non-essential fats carry these vitamins and alter them for cellular function. Using a water based or 'dry' fat-soluble won't alter the way fat-soluble vitamins act once they are absorbed. You still need the good fats and must be able to digest them to get them 'in'.
If you have had your gallbladder removed you no longer concentrate bile. You may need to take lecithin, about 1 heaped teaspoon of the granules, or a concentrated fat-digesting enzyme (lipase) or concentrated pancreatin or ox bile at every meal, especially meals containing your fat-soluble vitamins and omega-3 oils.
If you have difficulty digesting fats but still have your gallbladder using the lecithin or lipase or pancreatin along with 500 mg of taurine with each meal for a few weeks while getting the fat-soluble vitamins and omega-3 fats will most likely correct the problem. Use the digestive aids temporarily and see how you improve.
Nature's Sources AbsorbAid powder is an excellent digestive aid. Be careful to follow instructions. Powder mixes more freely with your food. Capsules or tablets (unless they are chewable) are not the best choice. My favorite lecithin granules are the Fearn brand. Use as much as you need to emulsify the fats. You can tell because the fats won't reflux and your digestion will proceed normally.
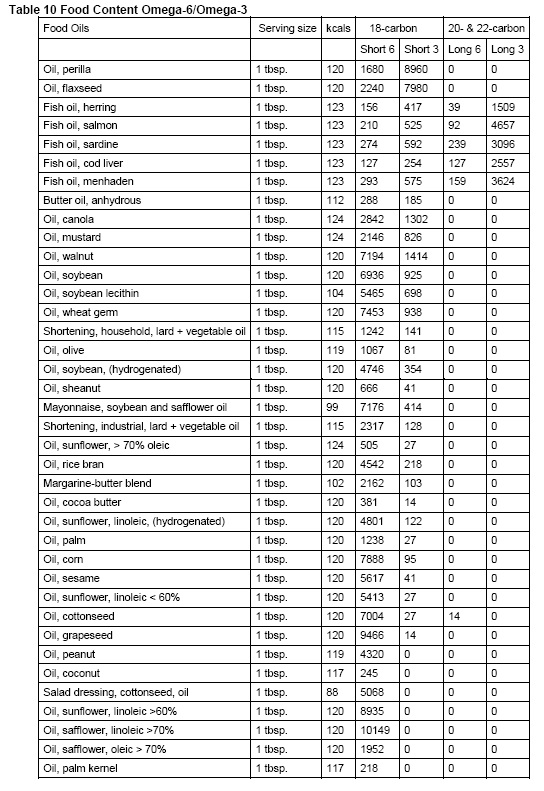
Avoid high Short 6 and get Long 3. Use only oils in bold. Use Olive, Butter and Coconut for cooking.
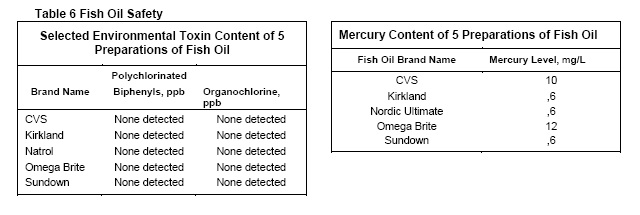
Regarding Fish and Fish Oil Efficacy and Safety
Mercury toxicity is not a consideration with fish oil. Mercury is WATER soluble, not fat soluble. Low fat tuna and the flesh (not fat) of other large fish contain the highest levels of mercury. Other toxins can be present in fish oils. Reputable manufacturers should be willing to provide safety standards/testing. Due to the way fish oil is processed many contaminates are removed and taking fish oil may be safer than eating large amounts of fish.
Farmed fish have the lowest levels of omega-3 and highest levels of ALL contaminants. Do not consume.
Some clinicians have suggested that only a particular brand or source of fish oil, usually one they are selling, is safe. They have reasons, often ones that appear to make sense, however, there is no evidence that fish oil from any of the major, reputable, companies is harmful or damaged. Now Foods offers Super EPA Double Strength, Ultra Omega-3 and DHA-500. These concentrates allow fewer soft gels to supply your daily need at reasonable cost.
If you use a particular source and you get results, have more energy, improved vision, experience improved memory, continue using your source, whatever it may be. Just make sure you get sufficient DHA, a full dose daily. If you haven't experienced the above benefits, consider a change. To confirm your choice get tested from OmegaQuant.
Some popular omega-3 choices on the web
krill oil
fermented cod liver oil
extra virgin cod liver oil
While krill oil does provide omega-3, like all of the core elements on this site, NUMBERS COUNT. We need, as humans, a particular amount of EPA and DHA and this amount should not be considered unimportant. While krill does contain phospholipids and may be better absorbed by some you still have many cells and many mitochondria, some 30-40 percent of those trillions of cells/mitochondria prefer omega-3 as DHA or EPA and less than enough won't do the job. Krill oil does not contain significant amounts of EPA and DHA and many soft gels would need to be taken to equal amounts recommended. Save your money AND SAVE THE WHALES. WHALES NEED KRILL OIL TO SURVIVE, YOU DO NOT. Buy reasonably priced fish oil, keep it in the refrigerator or freezer, and use it daily.
Fermented cod liver oil has some miraculous claims. It is likely not a bad product. It does not have a reliable amount of A and D. It is very expensive. If you like this and have another source for A and D and eat fatty fish, enjoy. There is no quality that makes it superior to other sources of DHA and EPA.
Extra virgin cod liver oil is even more expensive. It is likely all natural however the company has had some toxicity issues in other products. It does not have an established amount of A and D and taking enough to provide significant omega-3 would be prohibitive financially and perhaps unwise re unknown amounts of A and D meaning perhaps either not enough or excess A and D.
As to efficacy and safety I refer you to:
Measurement of Mercury Levels in Concentrated Over-the-Counter Fish Oil Preparations
Is Fish Oil Healthier Than Fish?
Stacy E. Foran, MD, PhD; James G. Flood, PhD; Kent B. Lewandrowski, MD
c Context.-Fish consumption has been associated with a decreased risk of coronary artery disease. Recent studies have illustrated that the high mercury content in cold-water fish may negate the cardiovascular benefits of fish meals. Fish oils have similar antiatherogenic properties to fish, and similar studies should be performed to determine the level of mercury in fish oils. Objective.-To determine the concentration of mercury in 5 over-the-counter brands of fish oil.
Results.-The levels of mercury in the 5 different brands of fish oil ranged from nondetectable (,6 mg/L) to negligible (10-12 mg/L). The mercury content of fish oil was similar to the basal concentration normally found in human blood.
Conclusions.-Fish are rich in omega-3 fatty acids, and their consumption is recommended to decrease the risk of coronary artery disease. However, fish such as swordfish and shark are also a source of exposure to the heavy metal toxin, mercury. The fish oil brands examined in this manuscript have negligible amounts of mercury and may provide a safer alternative to fish consumption. ( Arch Pathol Lab Med. 2003;127:1603-1605)
 |
Measurement of Organochlorines in Commercial Over-the-Counter Fish Oil Preparations
Implications for Dietary and Therapeutic Recommendations for Omega-3 Fatty Acids and a Review of the Literature
Stacy Foran Melanson, MD, PhD; Elizabeth Lee Lewandrowski, PhD; James G. Flood, PhD; Kent B. Lewandrowski, MD
c Context.-The consumption of fish high in omega-3 fatty acids is advocated by the American Heart Association to decrease the risk of coronary artery disease. However, fish contain environmental toxins such as mercury, polychlorinated biphenyls, and organochlorine pesticides, which may negate the beneficial cardiovascular effects of fish meals. Toxin levels vary depending on both the fish source and the specific toxin, and neither farm-raised nor wild fish are toxin free. Fish oil supplements also prevent the progression of coronary artery disease and reduce cardiovascular mortality. However, only sparse data exist on the level of toxins in fish oil. In a previous study we showed that the amount of mercury in 5 over-the-counter brands of fish oil was negligible.
Objective.-To determine the concentrations of polychlorinated biphenyls and other organochlorines in 5 over-the-counter preparations of fish oil.
Design.-The contents of 5 commercial fish oil brands were sent for organochlorine analysis. Results.-The levels of polychlorinated biphenyls and organochlorines were all below the detectable limit.
Conclusions.-Fish oil supplements are more healthful than the consumption of fish high in organochlorines. Fish oils provide the benefits of omega-3 fatty acids without the risk of toxicity. In addition, fish oil supplements have been helpful in a variety of diseases, including bipolar disorder and depression. ( Arch Pathol Lab Med. 2005;129:74-77)
Unless the 'expert' can show you data, hard data, not produced by them or offered second hand, but from an independent reliable testing or research source, to prove the 'danger' of some particular brand of fish oil please consider the above and this:
An affordable, fresh, clean source of the all important omega-3 fatty acids is better than an unaffordable source. It should not cost a fortune to maximize your health.
EPA and DHA do different things in our bodies. Both are important. Different omega-3 sources contain different balances between these two omega-3 fats. If you decide to take fish oil take a balance of both EPA and DHA. Many fish oils contain slightly or a lot more EPA than DHA. Always count the combined number of these two for total essential omega-3 per soft gel. An essential daily dose is 2,000 mg DHA plus near equal amounts of EPA. I prefer the balance to be in favor of DHA such as found in cod liver oil and the Now Foods DHA-500. Do not use a fish oil supplement that does not state exactly how much EPA and DHA it contains. The product you choose should contain near equal amounts of DHA/EPA. DHA can be converted into EPA but EPA cannot be converted into the very essential DHA.
Liquid or Soft Gels? While fish oil, as oil, is certainly more natural than soft gels, soft gels protect the oil from rancidity (destruction by oxygen). However fresh the fish oil may be when purchased, once your bottle is opened the process of destruction by oxygen progresses rapidly. Liquid oils are more exposed to this destruction. Unless you intend to finish the entire bottle of liquid fish oil within two or three weeks (the liquid oil not the oil in soft gels), consider the soft gels as a safer source. Cod Liver Oil has a longer refrigerated shelf life because of the anti-oxidants A and D. Just over a month should be consider still 'fresh'.
If using Cod Liver Oil as all or part of your omega-3 daily dose make sure you do not get more than 10,000 IU vitamin A from any/all sources. It is unlikely you will be able to get your full DHA dose safely using regular (not the Carlson) cod liver oil as your single source. Over time larger doses of vitamin A will be a cause of concern.
After opening your bottle of fish oil store the oil or the oil in soft gels in your refrigerator or freezer to help either stay fresh longer.
Remember when reading labels to make sure the number you are using is per each. Many labels give the number for 2 or some other serving size and you will need to take that into consideration when running the numbers.
For obese persons the upper limit of supplemental omega-3 is probably 6,000 mg of combine EPA-DHA no matter your weight. Higher doses of fish oil may cause digestive distress and show no more benefit than somewhat lower doses This would be 10 of the Now Foods Super EPA Double Strength or 7 of the Now Foods DHA-500 or 2 tablespoon Carlson Cod Liver Oil. Maintenance after 8-12 weeks of repletion would be 2,000 mg DHA plus whatever EPA is present in that dose.
There is strong evidence omega-3 DHA alters genes necessary to 'burn' fat. Recent research from Japan found increasing omega-3 DHA induced genes that shift metabolism to fat burning rather than fat storage. An increase in DHA/EPA converted white fat from lipogenesis (storage) to beige fat lipolysis (burnable). This is critical for anyone with diabetes, heart disease, thyroid disease and for everyone worrying about weight, that mid-line spread after 40. Fat is energy but it cannot be burned efficiently without sufficient body content of DHA omega-3.
Often within the 'health food' community I get the feeling from advertising promotion (by book sellers, alternative physicians, health food store personnel and others) that we will surely perish unless we spend large sums of money to purchase every new 'discovery' in a bottle. Health still comes from regular exercise, good food, good friends and joy in life. These things will never be bottled.
What is required is the daily consumption of FOOD, containing all essential fats, protein and fiber. This looks like-
Whole vegetables GROWN WITH LOVE IN MICROBE AND NUTRIENT RICH SOILS in great quantity, providing fiber, carbohydrates, vitamins and minerals
Whole fruits in season, GROWN WITH LOVE IN MICROBE AND NUTRIENT RICH SOILS providing fiber, carbohydrates, vitamins and minerals
Adequate proteins naturally found with healthy fats as found in WILD CAUGHT FISH, shellfish, fish roe (eggs), grass fed beef, pastured pork, lamb, wild game, poultry, eggs, organ meats, and if dairy tolerant, full fat dairy, including cheese, cottage cheese, quark, full fat yogurt and full fat kefir.
Few added fats including butter/ghee, extra virgin olive oil, and for some non-hydrogenated lard or coconut oil.
Fatty acids found in foods are critical to the health of all cells. Every cell membrane is composed of fatty acids and the human nervous system including the human brain is composed of numerous lipids making up between 60 and 70% of the total weight. These lipids are composed of dietary essential fats, both saturated and unsaturated. What fats you consume are critical to both your vitality and your longevity.
Fat is not the enemy but too much or the wrong types of fats will make you miserable (increase pain and inflammation, cause depression, contribute to obesity) and shorten your life. Check your refrigerator and your cabinets and toss out 'bad fats' and foods containing 'bad fats'. Stock up on the good fats and make sure to keep them fresh. You will appreciate the worth of your efforts within weeks. Omega-3 DHA will replace in brain cells in just 4 weeks, improving mood and even enhancing your hearing and your color vision. A reduction in omega-6 fats while increasing omega-3 fatty acids will improve muscle strength, reduce muscle and joint pain, and shorten exercise recovery time in just 3 months. Continued use will promote energy and, over time combined with a good diet and regular exercise reverse metabolic syndrome and obesity.
This page last updated: 08 September, 2024